While Bodie has been settling into a little bit of stability, health wise, and focusing on growing (pretty sure he just passed me up, but we’re not talking about that right now), I took a much needed weekend away for a cardiac networking conference and to see my girl!!!
The semi-annual Single Ventricle Outcomes NEtwork (SV-ONE) Learning Session was in Indianapolis this past weekend. (SV-ONE is a learning health network dedicated to transforming outcomes for individuals living with single ventricle heart disease (what Bodie was born with) across the lifespan. Through my work with Sisters by Heart, I have been involved with SV-ONE for some time now. It is an incredible organization and it’s always such a privilege to work alongside such dedicated practitioners, adult survivors and caregivers to make true change in the way individuals with single ventricle hearts live and thrive!)
Since I was so close to Sierra, I had her come up and join me for the conference (being pre-nursing, I thought she’d find it interesting), and then I went down and spent a few days in Bloomington with her.
What a joy it was to see her in her element!
I got to meet her friends, fill their (tiny) dorm fridge with groceries, fill their bellies with real food (apparently dorm food is getting old) and just give them some mama love.
I loved every second of seeing my girl! She has already grown so much and is absolutely flourishing at Indiana University. I could not be more proud of her. We suspected she would do well, but she has just blown me away! She is loving college life, focusing on her studies and really making Bloomington her home. And she has done it all while adjusting to a myriad of health issues, including an official diagnosis of both Hypermobile Ehlers-Danlos Sydrome (HEDS) and Mast Cell Activation Syndrome (MCAS), both of which have had some pretty nasty flare-ups since arriving in Bloomington. I am amazed that she’s able to concentrate on her studies while dealing with her symptoms!
When I first saw her, ALL that she wanted was Cheesecake Factory. Despite my argument that it was the LAST thing I needed at 9pm at night, I relented, Because…well…my girl wanted it!
In Bloomington, I took Sierra and her roommate to an IU Hockey game and it was SO FUN! (and just a little bit violent – ha!)
She walked me through campus, showing me the routes she takes to her classes. I was a business major, so didn’t spend much time over on the side of campus where her classes are. So I got to see parts of campus I hadn’t seen before (as a former tour guide, that says a lot)!
How gorgeous is this???
This is my absolute favorite time of year in Bloomington!
This girl is definitely her father’s child. All about the BBQ.
We discovered this place when we dropped her off for school and she begged to go back.
She introduced me to pretty much the best donuts I’ve ever had. AHMAZING!!!
A run to the grocery store with her roommate and another bestie. (Have I mentioned how fantastic her friends are??? She has sought out and found the best set of friends – they are all kind, driven, respectful girls who are GOING PLACES, let me tell you!)
I loved learning about the backgrounds of her friends, what they were studying, their families, etc. One of my favorite things was listening to Sierra describe her grandma (my mom) to her friends. She said “Did you guys read the Fancy Nancy books as a kid? Well, she’s like Fancy Nancy if Fancy Nancy were a grandma!!!!” Honestly, it’s the best description I’ve ever heard of my mom! She nailed it! If you know my mom, you’ll totally get it.
It was such a privilege to get a peak into her life, and it is not lost on me how lucky I am that she wants to bring me into her life at college!
I’m waiting at the airport now for the trek back home cross country. I’m not gonna lie – it was hard to leave my girl again. SO HARD. But it was so worth it to get to see her and how well she’s doing!
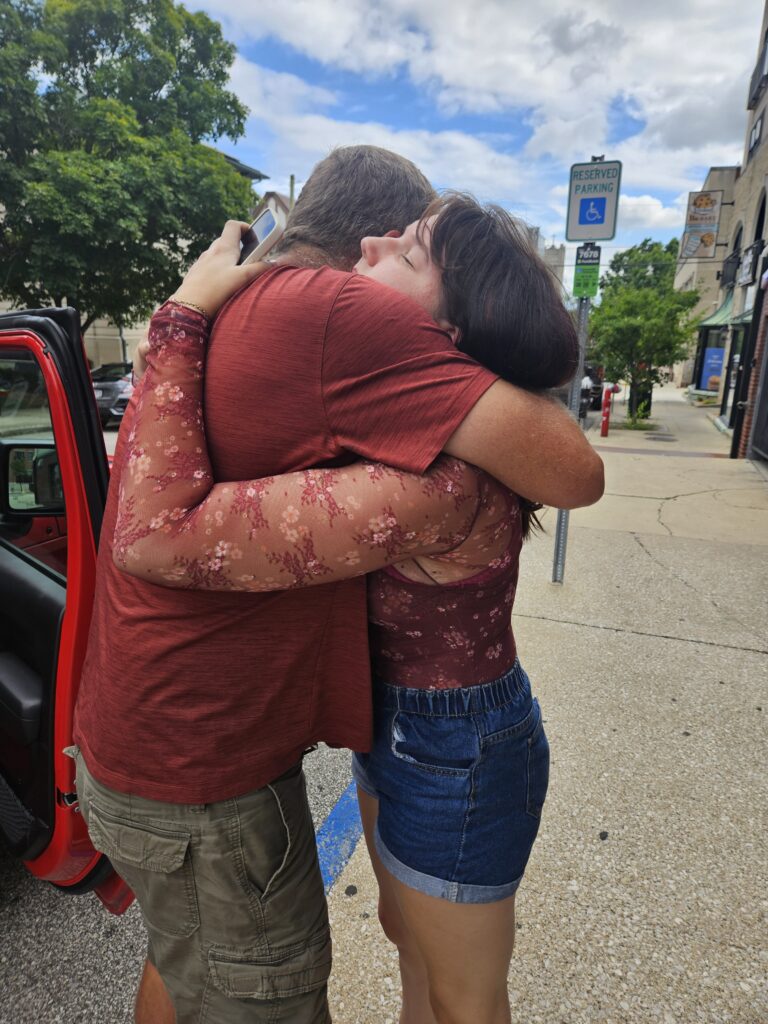
I grabbed as many hugs and kisses as she would allow, to fill my tank until I get to see her again – at Thanksgiving!!! (I may or may not be counting down the days!) Praying for a smooth rest of the semester for my girl!
Bodie’s appointments at Stanford went GREAT! As I mentioned, they can’t see everything with a CT scan that a cath will show, but between the blood work and what they COULD see on the CT scan, they’re very happy with how Bodie looks. As long as continues to look good clinically from the outside, we don’t have to go back until winter break for a cath and biopsy!
I should have known it was going to be a good trip when we got off the airplane in San Francisco and Bodie was moving so quickly I could barely keep up with him through the airport. I was reminded of the last time we flew into SFO and we ended up driving home 3 months later. I had to stop to take a comparison picture and was blown away just looking at the picture of him from last year.
I don’t remember him looking that sick.
Dusk doesn’t remember him looking that sick.
Our friends remember seeing him he week before and he looked fine.
But pictures don’t lie.
His decompensation happened so quickly – in a matter of days.
I remember once hearing that the problem with kids with heart defects is that they’re really good at compensating – until they can’t anymore. And they go downhill really fast when that happens. And that clearly was what happened to Bodie last June.
After all of his appointments, we hit up some of our favorite spots, including this random humane society park with this huge heart sculpture.
We have stopped there every time we’ve gone up!
We also went to this hill, which doesn’t look big.
But it is VERY STEEP. Last summer, during transplant recovery, I worked really hard to convince Bodie to try to walk up it once. He grumbled the whole way. But two days ago, he and I walked up it, and then down it, and then he asked me if we could run up it. So we did – and you guys, I could not even keep up with him!
It’s incredible to see the growth he’s had in the last year, but really in the past few months. It’s as though his body is finally settling into life with this new heart.
We still have a big open question of treatment for his platelets. His platelets on Thursday were actually 150K, which is the low end of NORMAL! So he is definitely responding to the injections. I think our next step is getting him to some degree of consistency so we know how much medication he actually needs, and then we can discuss trying to switch to the oral medication. Switching him to the oral medication will mean stopping the statin he’s on, and not every patient responds to the same way to the oral medication – and it comes with lots of dietary restrictions. So lots of hurdles to get through first. So for now, we’re still looking at weekly visits to Radys for lab draws and injections. But at least his platelets are improving, which means we’re in much better shape than a few months ago!
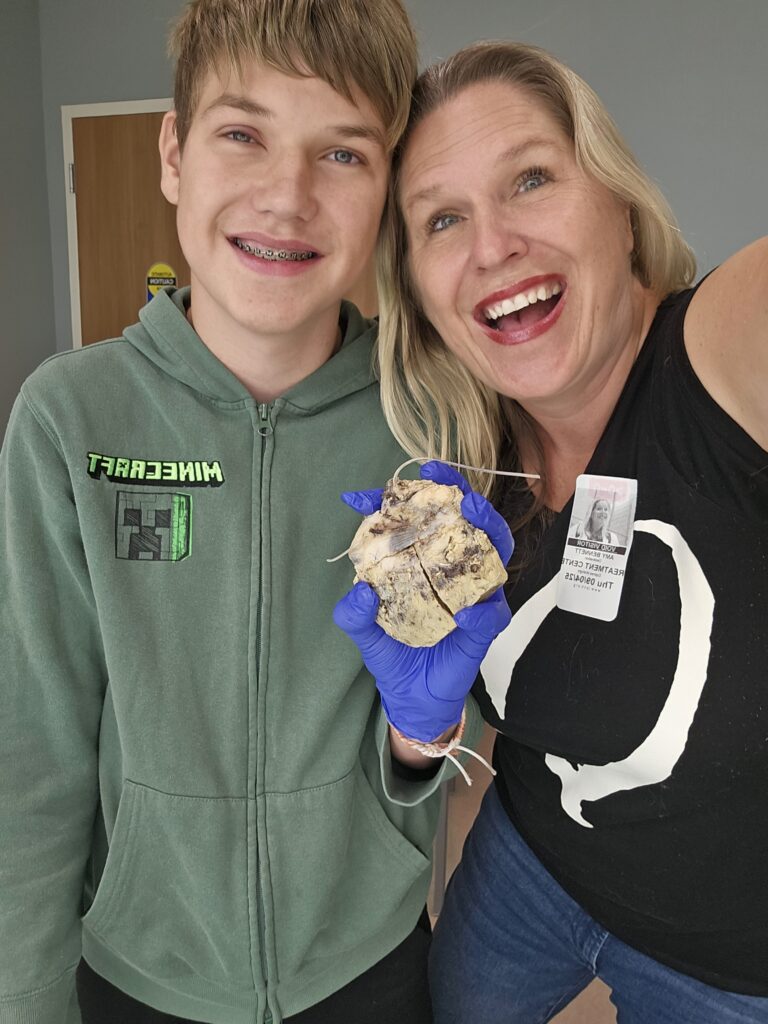
The most meaningful part of our trip by far was the opportunity Bodie and I had to go to the Pathology department and see Bodie’s old heart!
LPCH is one of the few hospitals that will allow transplant patients the opportunity to view their old organ, hold it, and ask questions. The doctor who led our session was incredible and had studied up on single ventricle hearts, so she was able to really explain to us all the ways Bodie’s heart was different than the typical heart we got to look at alongside it.
For me, it was such a moment of gratitude and wonder, to see that heart and how hard it had worked. The scars all over it were evidence of just how much has to be done to these single ventricle hearts to get them to function. For Bodie, I think it was very cathartic, not just to say goodbye to his heart, but to realize exactly how bad his heart was. It wasn’t enlarged as a heart in end stage heart failure would be. But as Bodie said, it looked “well seasoned” with so many scars. It truly looked like someone had MacGyvered it to get it to work, like they just grabbed whatever they had on hand at the time. It was kind of overwhelming to see it and really take it in. But overwhelming in a wonderful way.
If you’re not squeamish and would like to see a little of what we experienced (Bodie and I were there in person and Dusk and Sierra were able to Facetime in), check out the video I put together:
One thing we have learned unequivocally in Bodie’s heart journey is that when the hospital calls, we go…we drop everything and go…
Bodie’s team at Stanford has been nervously watching his weekly labs taken in San Diego, waiting to see if his platelets would stabilize so that we could move forward with his annual monitoring (which is now almost 3 months overdue). Unfortunately, we seem to have found the one thing in the world more stubborn than our son – his platelets!
His platelets ARE in a better range, but still bouncing around like they’re on the world’s most fun roller coaster. In the last 5 draws, they’ve been 27K, 70K, 23K, 100K and 79K. As a reminder, he needs to consistently be above 50K to even consider doing a cath and biopsy.
Because we’re already 3 months past when we were supposed to do these procedures, Bodie’s team is getting understandably nervous about wanting to see what’s going on inside his heart.
It’s not safe to do a cath and biopsy (which is more or less the gold standard of transplant monitoring). But his team doesn’t want to wait any longer to see what’s going on. So they’ve put together a less invasive monitoring plan, which includes a CT scan, Allosure Heart mapping and bloodwork, along with a multi-disciplinary clinic visit, EKG and echocardiogram.
All of this is designed to get us as comfortable we can safely get under our current circumstances. with Bodie’s heart, with a plan to follow up with a cath once we can safely do so. There are things we WILL NOT be able to do with a CT scan, like getting a good look at his coronary arteries and being able to biopsy his heart tissue.
It’s not perfect.
But it’s what we got.
So Bodie and I are headed up to Palo Alto for a couple of days of testing and appointments.
Please keep Bodie in your prayers:
Pray for his heart. Please pray that they see NO signs of rejection with this special heart. Bodie looks SO good from the outside these days – please pray that he looks as good on the inside as he does on the outside.
Pray for a clear path ahead. Given Bodie’s platelet situation, we’ve sort of been in limbo, treating the platelets but still not having a clear indicator (1) what is actually causing the issue, (2) what our long term treatment plan will be, and (3) how soon we can do a full cath and biopsy. Please pray we get more clear answers over the next few days.
Pray for Bodie’s spirit. He’s been pretty bummed to be back at school and already facing missing classes for medical appointments and procedures. (As a point of clarification, he is NOT sad about missing school – this kid does not like school! – he’s sad about constantly being behind in his schoolwork because of it.) Last year was a VERY hard fought battle for him, and left him discouraged toward school. Please pray for him to focus on the positives and how much better he feels.
Pray for smoother sailing. Bodie’s had a bit of a rough go of things in the first year post transplant. We covet smoother days ahead with fewer procedures and appointments, so that he can get to what 15 year old boys love to do – game and hang out with his friends!
I like to refer to Bodie’s transplant summer as Sierra’s “soft launch.” Completely unexpectedly, I was forced to learn to live 500 miles away from my sweet girl last summer, as she got a crash course in independence and forging her own way.
I thought that prepared me for this week, her hard launch, as we dropped her off at college.
In a way, I suppose it did.
But even so, walking away from this girl, everything we have poured our hearts and prayers into over the last 18 years, and leaving her 2,000 miles away, was hard. It felt surreal. It’s as though our hearts are bursting and breaking at the same time.
Bursting with pride over how ready she is, how brave this decision was, how many wonderful moments lie ahead for her.
But also breaking with sadness over an era over, a family life that will never be the same.
I turned to Dusk as we walked into the airport this afternoon and said through tears “You know how when you read a really good book, or play a good game, or listen to an amazing record and you get to the end, you want to immediately start it all over again? That’s what dropping her off at college felt like.”
And then I had to stop and modify my thought a bit, as I’d love to start all over again, but maybe skip over the teaching her to read bit, and definitely the potty training part…also, not sure I’d have the energy to do the toddler years again.
So, yeah, lot of mixed feelings. For both Dusk and I.
But I read a quote earlier today that really resonated with me – “Healthy birds fly the nest.” I’m choosing to ruminate on that in moments of sadness and emptiness.
But our girl? She’s gonna do great.
She’s moved in, and settled, and already exploring her new home with her roommate, a sweet girl from Georgia.
We think she has most of what she needs (even, yes, a pillow of her beloved Toulouse to watch over her). And whatever she realizes she needs, she’ll find out how to get.
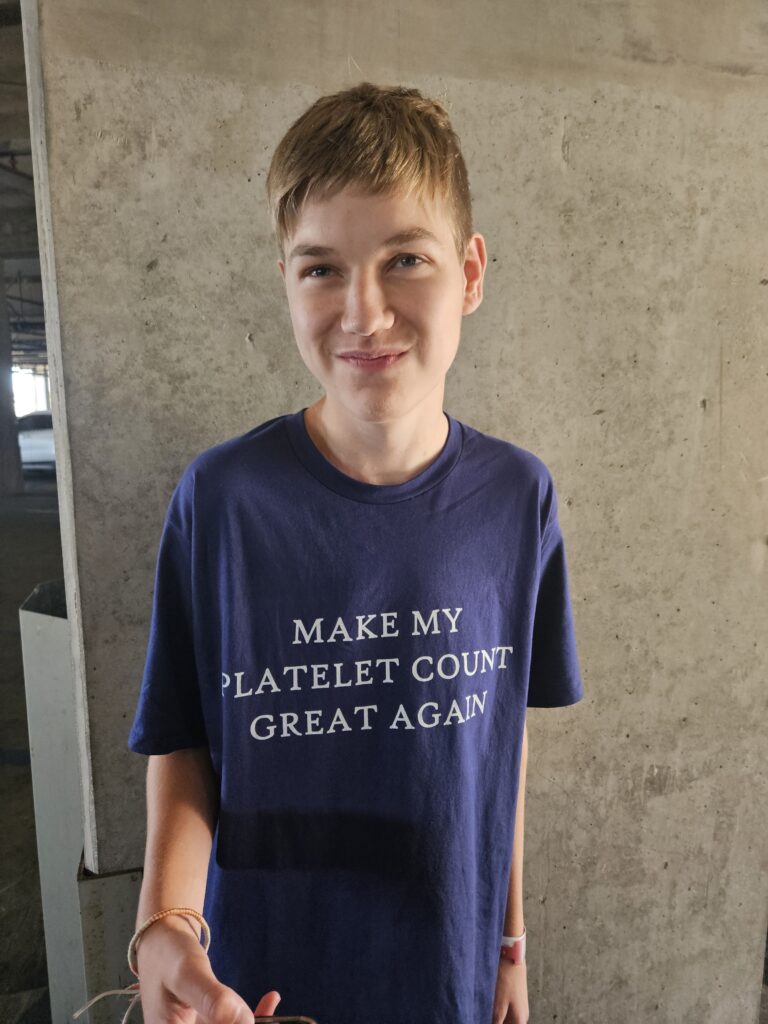
I put on my big girl panties and my brand new tee shirt and got ready for the goodbyes.
I did pretty well and didn’t cry until we left. The final hugs goodbye were hard, for both Dusk and I.
We hugged her and prayed over her, asking God to continue to protect her and guide her.
And then I cried a little more.
And we waved goodbye as she and her roommate giggled together and wandered into a darling vintage thrift store bearing IU clothing…and the start of her new life.
Spread those wings and fly, my sweet girl. You were made for this.
Just don’t forget to come back home once in a while to tell us all the things you see out there.
I’ve been meaning to write this post all summer, but kept delaying it because I wanted to wait to write it until I had something to post about Bodie’s ITP treatment. And, that, unfortunately, didn’t really improve until the end of the summer.
This kid has been such a trooper.
We’ve been making weekly trips down to Rady Children’s Hospital for labs and N-Plate injections for his ITP. After seeing an initial little jump to 25,000, his platelets leveled out in the 20,000s by early July, and sat there until last week. As a result, we weren’t clear to go to Stanford for his annual cath and biopsy, or to Tahoe for our annual family vacation…or anywhere, really.
It was a better summer than last summer, to be sure. But let’s be honest – that bar saw set pretty low. Even so, Bodie was bummed. He just felt like he lost 2 summers in a row. We did what we could – we played a lot (and I mean A LOT) of Pokemon Go with him, driving to local community meet-ups and walking a lot to catch cool creatures. He managed to get Dusk and I almost as addicted to Pokemon as he is (almost). We also tried to do fun things like trips to Menchie’s (his absolute favorite) after his appointments.
Since he had stabilized at 25,000 without major bleeding incidents, his Hematologist cleared us to do a day at Seaworld. She cleared him for all of the nonagressive rides. I’m not 100% sure her definition of nonaggressive is quite the same as ours, and we probably took a few liberties, but it was so worth it to see this smile!
We also got to take a 3 day trip to Palm Springs last week, which was a wonderful respite. Not nearly long enough, but at least we had an opportunity to take a break from work and spend some quality family time together.
At Bodie’s appointment last week, he had finally hit max N-Plate dosage, and his platelets had jumped to 70,000! It was amazing and exactly what we were hoping to see happen! His doctor was so excited. We’re hoping that’s where they’ll sit now, and it’s exactly where they want him as long as he’s getting the injections (normal is 150,000-400,000, but with patients on platelet stimulating medications like N-Plate, they don’t want them that high due to risk of overcoagulation.
Now we wait to make sure they stay in the range we want.
Then, we can go to Stanford for his annual cath and biopsy (they had been planning on doing something less invasive due to his lower platelet count, but now that he’s higher, I think they’ll want to do the regular annual testing).
After that, it’s anyone’s guess what the next steps are. N-Plate isn’t really a long-term solution, as driving an hour to the hospital every week forever isn’t exactly a good quality of life. If the medication continues to work well for him, we can consider switching him to an oral version of it, but it doesn’t always work the same as N-Plate, and there are dietary issues with it (calcium affects absorption of the medication). So we’ll hold off on that discussion for now. One step at a time. His team may also consider switching up his immunosuppressants to see if they’re causing the ITP. But before doing that. they’d need to do a cath and ensure everything looks good with his heart. Preservation of this special heart is our most important goal. Everything else comes second. So, again, one step at a time.
In the meantime, we’re breathing a little easier, even if it meant Bodie didn’t get the summer he wanted. He’s experienced a huge growth spurt, gaining 25 pounds since April and at 5’9 1/2″ is neck and neck with me (and is now shaving, but I didn’t tell you that)! His body is clearly in a happier place right now.
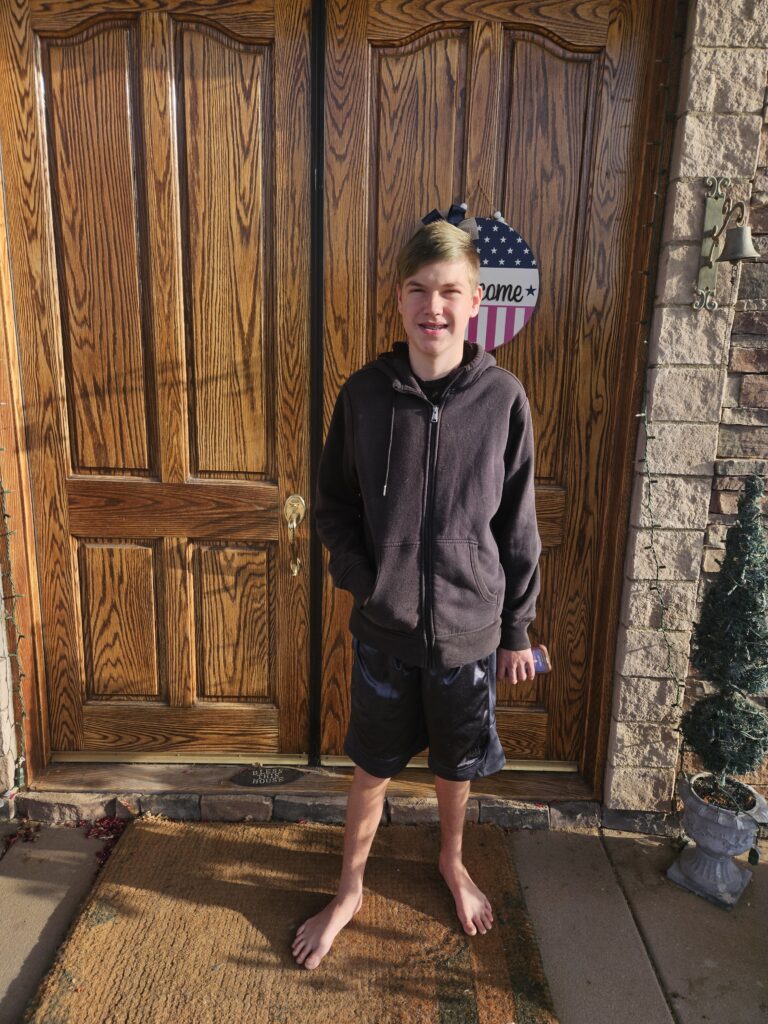
He started school last week. In true high school boy fashion, he refused a good first day of school picture. This was the best I got.
Wouldn’t even put his shoes on. But I’m choosing to pick my battles.
He’s cleared for heart camp, and we drop him off for that next week. But first, we drop his sister off for college! Big changes around the Bennett household.
We covet your continued prayers that Bodie’s platelets stay in range, further interventions won’t require him to miss much school, and we all adjust to our new family dynamic with Sierra off to college!
Our life has been pretty chaotic as of late. In the past 3 weeks Bodie had an emergent unplanned hospital admission, got out in time to take his finals, fought with me for 3 days straight about taking said finals, Sierra graduated, we had a family graduation lunch, we hosted a graduation party at our house for 50 people, Sierra got in a bad accident on the way to graduation and totaled Dusk’s car (no one was seriously hurt, thank God, but we’ve been dealing with insurance and the rental car company), Bodie was readmitted to the hospital and I threw my back out…needless to say, it’s been a lot.
I have lots to update on (including Sierra’s graduation!), but that will need to be a post for another day. So many of you have been asking me how Bodie is, so I wanted to update. It’s been a lot to process, which is why I haven’t been updating on the blog. (Also, due to the recent events, my life has been too crazy to find time to sit down and blog. Ha). But here goes…
As I mentioned previously, Bodie has been diagnosed with ITP (Immune Thrombocytopenic Purpura) a rare autoimmune disorder where the body’s immune system mistakenly attacks and destroys platelets, the blood cells that help with clotting. As a result, he could start internally bleeding at any time, and doesn’t clot well when he injures himself.
ITP is an extremely frustrating condition to treat, because every patient’s cause is different and treatment plan is different. The treatment for ITP essentially involves going through the protocol of possible treatments from least invasive to most invasive, until you land on the one that works for your child.
It is, unfortunately, not a condition that is diagnosed and resolved within a week or two.
So we have to be patient while they work through the possible treatment plans, to find the one that works for Bodie.
Treatment 1. Platelet Transfusion. When a patient presents with ITP, the least invasive line of treatment is a platelet transfusion. It’s exactly what is sounds like: it’s just like a blood transfusion, except it’s platelets instead. In Bodie’s case, his platelet antibodies are so high that this treatment was wildly unsuccessful. His antibodies attack the platelets as soon as they’re in his system. In fact, his platelets actually decreased after his first platelet transfusion. They increased slightly when they used a platelet batch actually matched to his antibodies. Both of those transfusions were done during his first hospital admission in late May/early June. They didn’t even attempt a platelet transfusion during his admission last week.
Treatment 2. Steroids. Steroids tend to be a first line treatment when the body has an overactive immune response. Bodie has had luck with Decadron (a corticosteroid medication with the active ingredient dexamethasone), as it both treats ITP and helps modulate side effects of IVIG. So he’s done 4 day courses both times he’s been inpatient recently. But to do it at full treatment dosing would be a higher dose for a longer period. Dusk is extremely steroid sensitive – 1 week on Prednisone caused Avascular Bilateral Hip Necrosis, and he had to have both of his hips replaced at 37 years old. Bodie does not appear to have a steroid sensitivity, but we didn’t discover Dusk’s until he was in his 30s. So we’re always very conservative with steroid use with Bodie.
Treatment 3. Intravenous immunoglobulin (IVIG). is a treatment where a concentrated dose of antibodies (immunoglobulins) from donated blood is administered intravenously (through a vein). IVIG helps to boost or modulate the immune system, providing antibodies to fight infections or regulate overactive immune responses (the latter is essentially what is happening with Bodie). IVIG is also used to treat Donor Specific Antibody rejection, which Bodie had pop up on a blood test a few weeks after his transplant. So he had several rounds of successful IVIG treatments last summer at Stanford. During his first admission in late May/early June, he seemed to be the most responsive to IVIG. They did 2 back to back IVIG treatments during that admission, and another 2 back to back treatments during last week’s admission. It does seem to give him a temporary boost, but definitely does not give him enough to last. (When we left the hospital after his first admission, his platelets had jumped up to 43,000; 3 days later, they were back down to 7,000).
Treatment 4. Nplate Injections. Nplate (romiplostim) is a prescription medication administered via subcutaneous injection into the body to stimulate platelet production. The goal is to stimulate the body to produce enough platelets that they overwhelm the overactive antibodies. Bodie had his first injection last week. The injections are done on a weekly basis in the Hematology clinic in the hospital. Full dosage is 10 units. They can start patients anywhere between 1 and 3 units. They started Bodie at 3 units, and will go up 1 unit a week until he is at full dosing. Unfortunately, they cannot be administered at home or at a satellite facility, because each week his platelets will need to be checked first, and then the injection will be titrated specifically to his platelet level. So we’ll be driving an hour to the hospital for these injections for the foreseeable future. The tough part about this one is that we won’t know for awhile whether or not it is working. Some kids show a response in as little as 3 or 4 treatments, but most have to get to full dosing to really see an effect. (Side note – there is an oral medication that does the same thing, but it interferes with his Statin medication (transplant patients are on statins as they seem to be the best way to prevent Coronary Artery Disease, which is the biggest reason for re-transplant), so the oral medication is off the table for Bodie, unfortunately.)
Treatment 5.Bone Marrow Biopsy. This is really more of a diagnosis tool than a treatment, but I put it on the list as it’s the order of the protocol. If the Nplate injections do not prove successful, they’ll likely want to look at his bone barrow to get a better look at what exactly is going on to ascertain which treatment might make the most sense.
Treatment 6. Change immunosuppressant medications. If the bone marrow biopsy comes back normal, we would move on to looking at which if his medications could potentially be causing Bodie’s ITP. The challenge with Bodie is that any of the medications he is on – Tacrolimus, Everolimus and Valganciclovir – all could potentially cause ITP. Tacro is the most likely, but either of the other two could cause it as well. Because the Valganciclovir is actually an antiviral, used to treat/prevent CMV and he’s had several negative CMV tests at this point, we are going to trial off of that one this week. But the Tacro and Evero are here to stay unless or until we hit this treatment step. Changing up immunosuppresants is not for the faint of heart, and requires a lot of very careful slow titration up and down of medications, so would likely need to be done inpatient at Stanford.
So where does that leave us?
In a lovely holding pattern.
We’re currently on Treatment 4, the Nplate injections. And we might not know for a couple of months whether or not it’s working.
So for now, we see the Hematologist weekly where they check his platelets and give him the injection.
And we make sure he doesn’t engage in dangerous (you know, normal 15 year old boy stuff) behavior. No biking, skateboarding, contact sports, etc. For once, I’m glad he’s a gamer and not an athlete!
And we watch and wait for him to bleed.
Because he will.
When he was discharged from the hospital last Friday, his platelets were at 10,000. Again, nowhere near the normal range of 140,000 – 440,000. But as long as he’s not “actively bleeding,” we can stay home.
When (and I say if, not when, because we know he will) he starts to bleed, it’s likely be in the form of a nosebleed, or mouth bleeds, or blood in his stool or urine. And when that happens, we call his Hematology team. And they decide whether we’re close enough to his next clinic appointment to stay home. Or whether we need to come into clinic for a 6 hour IVIG treatment. Or whether we need to be admitted for treatment.
Meanwhile, with platelets hovering in the single digits, he’s not safe to make long road trips (if we were in a car accident, the consequences could be devastating) or to fly (if he were to bleed in the air we would have limited options to treat it).
So his annual biopsy and cath at Stanford (previously scheduled for tomorrow) have been postponed, along with his follow up appointment with his ENT and his viewing of his old heart with the pathology team. And our planned visit to Alcatraz. He’s not safe to do the procedure right now, let alone to travel there. We don’t know yet when they’ll be rescheduled.
And our trip to Tahoe in two weeks will likely also be postponed. We do pretty low key stuff while we’re there, but it’s the getting him there that wouldn’t be safe.
Needless to say, we have a pretty sad boy.
He says he’s “going to Tahoe anyway. The doctors can suck it up.”
While I appreciate his tenacity, unfortunately, it doesn’t quite work that way.
So we covet your prayers.
It is not out of the question that the ITP could spontaneously resolve – completely unlikely, but God has done the ridiculously unlikely with Bodie before and he can do it again. So please pray for that miracle!
Please pray that Bodie’s body responds far better than expected to the Nplate injections, and he’s in a safe space to travel soon!
We have been abundantly blessed that we have found an incredible Hematologist at Rady’s who works really well with our Stanford transplant team! She is so smart and works so collaboratively. Praise God for that! Please pray they continue to work well together to figure the cause of Bodie’s ITP out more quickly than anticipated!
Please pray that we can switch our Tahoe week for a week later in the summer. When we go, we’re in a timeshare, so can only go if we can swap it for a week later in the summer. It’s hard to plan since we don’t yet when he’ll be safe enough to go. Right now it’s not looking too promising. Please pray something magically opens up when we need it.
Please pray for my spirit. I’m feeling pretty burnt out and rundown right now. I’m a planner and we had a heavily planned summer that has now all gone up in smoke. I’m trying desperately to keep up with my client workload amidst all of this, but it’s hard working in the hospital, for a variety of reasons. So I feel like I’m just constantly running behind and not able to do anything very well right now. I just need some peace, honestly.
Please pray especially for Bodie’s spirits. He missed last summer because of transplant recovery and he’s had a rough year academically. All year, we’ve been talking about how we were going to make up for all of it at Tahoe this summer. We so want him to have a FUN summer where he can get some of that time back!
And one final note – if you’re still reading this! You have all been so generous in your donations – I can’t believe we’ve made it all the way to $79,109!!! I cannot tell you how much that has helped offset our medical bills, hospital stays, travel costs and Bodie’s prescriptions! You’d be shocked at how quickly all of this adds up! If you’re still being led to give, please do so! We’d love to hit $100K raised before our 1 year anniversary, which is almost here! We’re only $21K away, so we could totally do it! Gifts are tax deductible to you and will be available for Bodie’s transplant related expenses for life! Thank you!